Below are answers to the most frequently asked questions about anterior cruciate ligament reconstruction (ACLR) surgery. These are based on two decades of MOON Knee Group research following patients for ten years starting before surgery. This information is provided for you to discuss with your surgeon about how it might apply to your body and injuries.
ACL Tear Information
The World's Leading Resource for Improving ACL Injury Outcomes
Anterior Cruciate Ligament Reconstruction Surgery Most Frequently Asked Questions
- What Is the Anterior Cruciate Ligament (ACL)?
- What Are the Other Three Knee Ligaments?
- How Do ACL Tears Happen?
- What Are ACL Tear Symptoms?
- How Are ACL Injuries Diagnosed?
- What Happens in ACL Reconstruction Surgery?
- How Soon Can I Have Surgery?
- Why Does Recovery Take So Long?
- Can I Walk With a Torn ACL?
- How Much Ability Will I Recover?
- Can I Retear My Reconstructed ACL?
- Are Females More Likely to Tear an ACL?
- What About Partial ACL Tears?
- What Other Knee Injuries Might I Have?
- How Do I Maintain My Reconstructed Knee Over My Lifetime?
- What About Arthritis?
Related Content
Site Search
What Is the Anterior Cruciate Ligament (ACL)?

The ACL is one of four strong fibrous tissue bands called ligaments that hold together and support the knee. The ACL runs diagonally inside your knee between your thigh (femur) and shin (tibia) bones. Your ACL primarily keeps your knee stable when you turn, cut, twist and pivot. Unfortunately, it is the knee ligament most often injured. An ACL tear is one of the most common and devastating sports injuries.
What Are the Other Three Knee Ligaments?
In addition to the anterior cruciate ligament, the other three knee ligaments are:
- The posterior cruciate ligament (PCL) also links the thigh and shinbones inside the knee toward the back of the joint. PCL injuries are rare.
- The medial collateral ligament (MCL) connects the two bones outside the joint on the inner side of your leg toward your other knee.
- The lateral collateral ligament (LCL) runs on the outer knee opposite the MCL. It connects your thighbone to your fibula, the smaller bone in your calf.
How Do ACL Tears Happen?
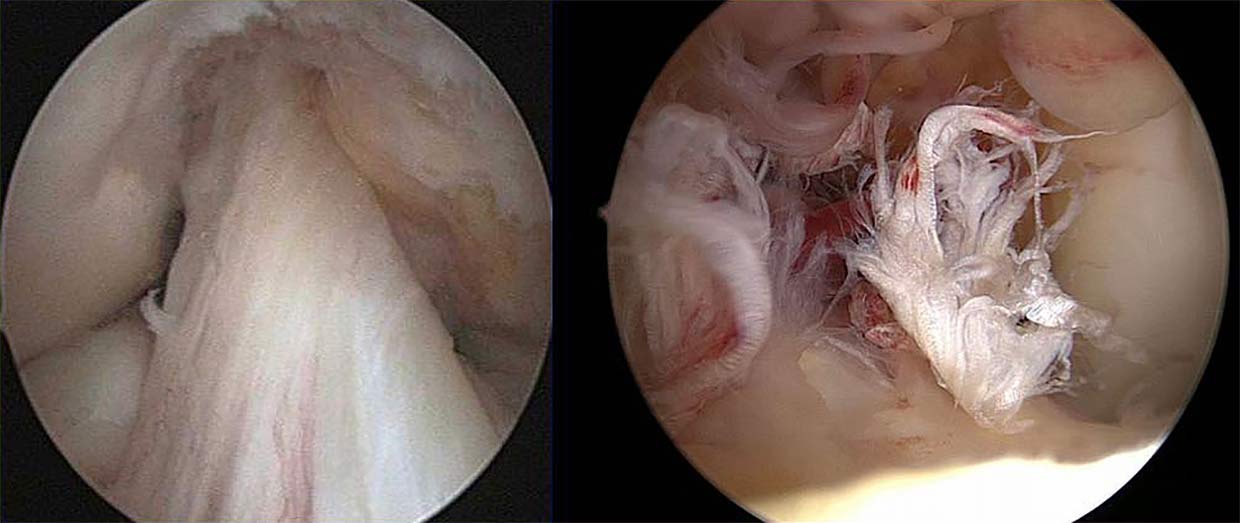
Unfortunately, your body can move in ways your knee ligaments can’t support. When that happens, the fibrous ligament tissues stretch or tear, as you can see in the image on the right. An ACL tear usually happens when jumping, turning or moving suddenly while running. Most of the time, the injury happens without contact. An ACL tear (also called a rupture) is the most common knee injury. More than 90 percent of the time, it tears completely.
What Are ACL Tear Symptoms?
When your ACL tears:
- Seventy percent of those suffering an ACL tear feel or hear a pop.
- You’ll feel pain that increases when you bend your knee or try to walk. It may hurt to put any weight on that leg.
- Usually your knee will swell quickly.
- Your leg might feel unstable. This is because your shin can move forward beyond its natural range (called loss of anterior stability). Also swelling and pain in your quadriceps (front of thigh) may keep the muscle from working properly.
- Your range of motion might be severely limited. It will be painful to straighten your leg.
How Are ACL Injuries Diagnosed?
ACL tears can be confirmed only through medical evaluation or magnetic resonance imaging (MRI). If you experience symptoms of a torn ACL, you should get a medical professional’s diagnosis as soon as possible to begin your recovery. A skilled musculoskeletal specialist can usually diagnose a tear by physical examination. An MRI confirms the tear and any other injuries in the knee. If your ACL is torn, you’ll be referred to an orthopedic physician and physical therapist specializing in knee injuries.
What Happens in ACL Reconstruction Surgery?
- You’ll be given general anesthesia. This means you’ll be unconscious during the operation.
- The surgeon makes two to three small incisions in your knee. These are for small arthroscopic instruments including lights and cameras that allow the surgery to be done without opening up your knee.
- The inside of your knee is flushed with sterile saline solution.
- The doctor inserts cameras and small tools and cuts and removes the torn ACL.
- One hole or tunnel is drilled in the femur. Another is drilled into your shinbone.
- A replacement tendon (called a graft) is placed in both tunnels and anchored with screws or sutures. In autograft surgery, the graft is taken (harvested) from your patellar, hamstring or quad tendons. In allograft surgery, the graft comes from a cadaver (see the retear risk calculators).
- Any other injury to your meniscus or other ligaments may be repaired at this time.
- The surgery lasts about two hours depending on the injuries in your knee.
- Patients go home the same day.
- Physical therapy begins within a few days.
How Soon Can I Have Surgery?
After an ACL tear is diagnosed, your knee will benefit from prehabilitation exercises. Research shows improved results—including for return to sport—when the following are true before ACL reconstruction surgery:
- Swelling is minimal.
- You can fully straighten your knee.
- You’ve recovered most of your normal knee bending or flexion.
- The muscles (especially the quadriceps) surrounding your knee are strong. Research shows weak quads at the time of surgery are usually weaker two years later.
This is the first of many times where you’ll be rewarded for being patient. You’ll benefit from getting your body ready before surgery, even if it takes a few weeks. There is no standard duration for prehabilitation as injuries and strength vary.
Why Does Recovery from ACL Surgery Take So Long?
- The knee is the largest joint in the body. It works in coordination with every other muscle and bone on that side of your lower body up through your back. The knee’s ability to support all activities, especially demanding sports, is astonishing. A knee injury is a big disruption to your body.
- The ACL is critical to stabilizing your knee.
- Very little blood circulates inside your knee, which slows healing.
- ACL surgery rehabilitation develops functionality and strength. Functionality is being able to do something. Strength is being able to do it with force. Strength takes longer to regain than functionality.
Completing a full step-by-step rehabilitation program improves your final result and reduces your retear risk.
Can I Walk with a Torn ACL?
Immediately after suffering a full ACL tear, walking will be uncomfortable at best. You will likely feel unstable. This is result of several factors:
- Loss of anterior stability (your shin can now move forward beyond its natural range)
- Swelling in your knee
- Pain keeping your quadriceps (front of thigh) muscle from working properly
Choosing to not having surgery? Eventually, you should be able to walk without pain after physical therapy. Note that deciding to not reconstruct your torn ACL usually means you have to permanently avoid aggressive cutting and pivoting.
How Much Ability Will I Recover?
Following reconstruction surgery and with full completion of rehabilitation and return-to-sport training, you can recover greater than 90 percent of your preinjury functionality as measured by commonly used sports outcome scores. However, this depends on your body, injury, graft choice and commitment to prehabilitation and rehabilitation. As you go through rehabilitation, continue to be evaluated and discuss your progress with your physical therapist and athletic trainer.
Can I Retear My Reconstructed ACL?
Yes. Even the best reconstruction surgery cannot eliminate the possibility of a retear. See the reinjury risk section and calculators to see how graft choice for your ACL reconstruction affects your retear possibility. You can reduce your retear risk by completing full pre-surgery (prehab) and post-surgery rehabilitation programs plus specific return-to-sport training.
Are Females More Likely to Tear an ACL?
Yes. Studies have shown females are two to seven times more likely to tear an ACL than males competing in the same sports. Theories for this difference between sexes range from hormonal and anatomical differences to lower biomechanic and neuromuscular control. This difference goes away after ACL reconstruction surgery: retear risk is the same regardless of sex.
What About Partial ACL Tears?
Less than 10 percent of ACL tears are partial. The extent of an ACL tear can only be confirmed through medical evaluation. If you do suffer a partially torn ACL, you might be able to recover without surgery. This could leave you at higher risk for full tear, particularly if you return to a sport involving jumping, cutting and pivoting.
What Other Knee Injuries Might Happen When I Injure My ACL?
When you tear your ACL, other parts of your knee can also be hurt.
- You might tear or strain other ligaments.
- The knee cartilage (meniscus) cushioning your knee may be damaged.
- Your kneecap as well as the smooth articular cartilage on the bottom of your thighbone and the top of your shinbone might have injuries like cracks.
- Tendons and bursae (small fluid sacs in the knee) could be inflamed.
A medical evaluation that includes an MRI will detect any other injuries. Most can be treated at the same time as your ACL. Your physician can discuss in more detail your injuries and treatments.
How Do I Maintain My Reconstructed Knee Over My Lifetime?
There is no research on maintaining your reconstructed ACL over a lifetime. However, common sense and nearly all medical and training professionals advise maintaining strength, range of motion and fitness with non-impact aerobic exercise.
What About Arthritis After ACL Injury?
Tearing your ACL, along with any other knee trauma, increases your chances of developing arthritis in your knee. This is likely to occur at a much earlier age than without the ACL tear.
Was This Content Helpful?

Share via: